
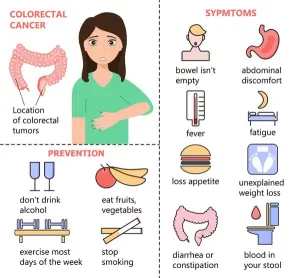
Colorectal cancers may present with:
However, most early-stage colorectal cancers generally have little to no symptoms when the growth is small. Hence, screening for polyps and cancers remains the single most effective strategy in decreasing the mortality from colorectal cancers.
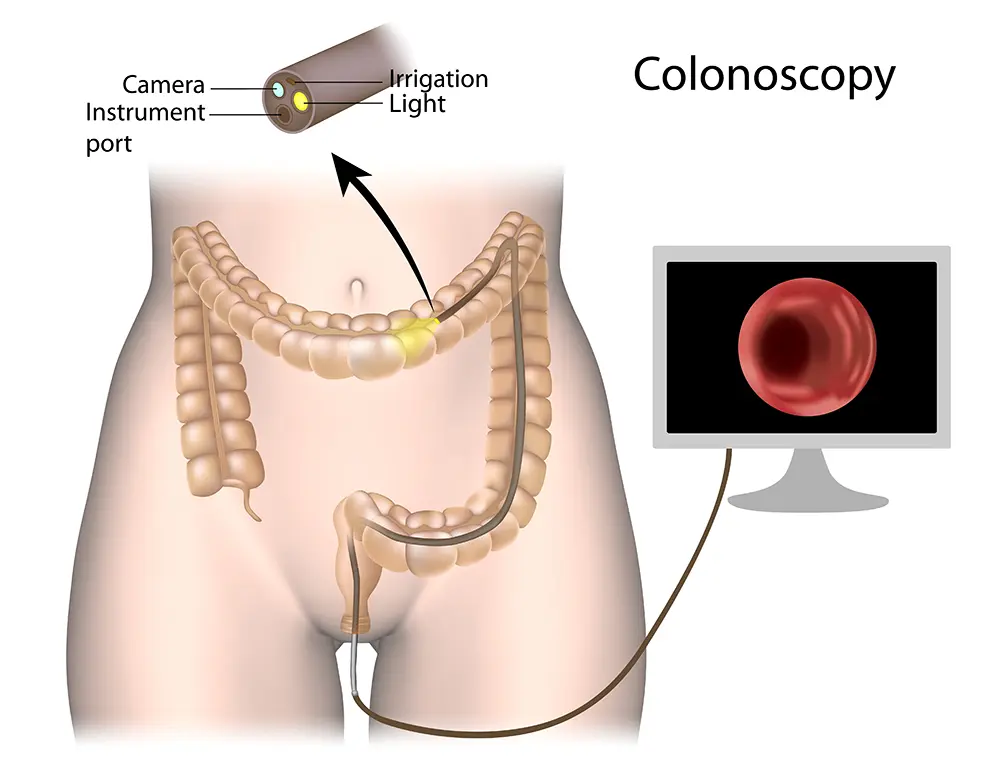
A colonoscope (flexible tube with light source at the tip) is inserted by a doctor through the anus along the whole length of the colon to look for polyps or cancers. Any abnormal spot can be sampled using a small instrument passed through the colonoscope. Light sedation is usually administered prior to the procedure to keep you comfortable.
 Appropriate treatment of colorectal cancer depends on:
Appropriate treatment of colorectal cancer depends on:
Stage 1 colorectal cancers are generally treated with surgery alone. Some stage 2 colon cancer with adverse features on surgical specimens may require chemotherapy after surgery (adjuvant chemotherapy) to reduce the risk of relapse. Patients with stage 3 colon cancers are generally advised to undergo adjuvant chemotherapy after surgery. Stage 4 colon cancers are generally treated with chemotherapy, targeted therapies or immunotherapy. Select patients with stage 4 colon cancer who have limited spread, especially in the liver or lungs, may be suitable for curative intent surgery /local ablation plus chemotherapy. Radiotherapy has a well-defined role prior to surgery in locally advanced rectal cancer, to improve local control and reduce local recurrence. It can also be used to ablate limited sites of metastatic disease.