
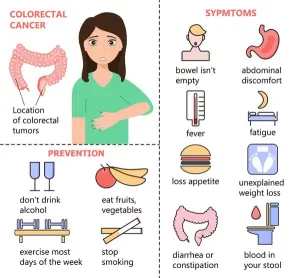
Ung thư đại trực tràng có thể xuất hiện cùng các triệu chứng sau:
Tuy nhiên, hầu hết các bệnh ung thư đại trực tràng giai đoạn đầu thường có ít hoặc không có triệu chứng khi khối u còn nhỏ. Do đó, tầm soát polyp và ung thư vẫn là chiến lược hiệu quả nhất trong việc giảm tỷ lệ tử vong do ung thư đại trực tràng gây ra.
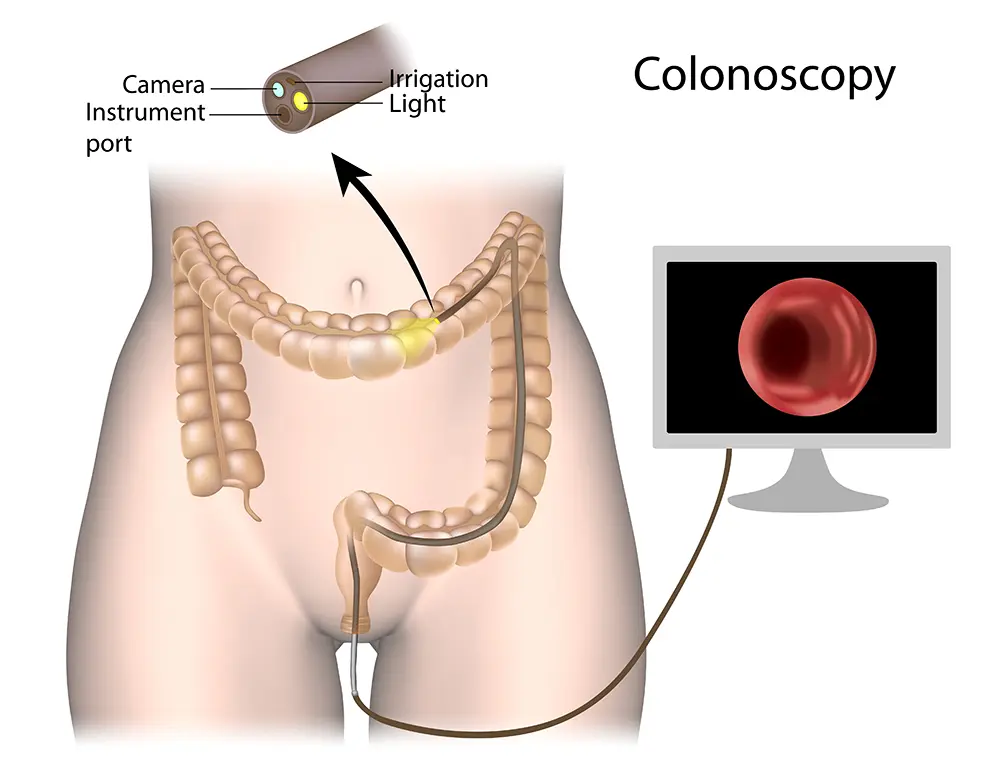
Một ống nội soi (ống mềm có gắn đèn ở đầu) được bác sĩ đưa qua hậu môn dọc theo toàn bộ chiều dài của đại tràng để tìm polyp hoặc ung thư. Có thể lấy mẫu bất kỳ điểm bất thường nào bằng cách sử dụng một dụng cụ nhỏ đưa qua ống nội soi. Thuốc an thần nhẹ thường được sử dụng trước khi thực hiện thủ thuật để giúp bạn cảm thấy thoải mái.
 Việc điều trị thích hợp ung thư đại trực tràng phụ thuộc vào:
Việc điều trị thích hợp ung thư đại trực tràng phụ thuộc vào:
Ung thư đại trực tràng giai đoạn 1 thường được điều trị bằng phẫu thuật đơn thuần. Một số trường hợp ung thư đại tràng giai đoạn 2 có đặc điểm bất lợi trên mẫu bệnh phẩm phẫu thuật có thể cần phải hóa trị sau phẫu thuật (hóa trị bổ trợ) để giảm nguy cơ tái phát. Bệnh nhân ung thư đại tràng giai đoạn 3 thường được khuyên nên trải qua quy trình hóa trị bổ trợ sau phẫu thuật. Ung thư đại tràng giai đoạn 4 thường được điều trị bằng liệu pháp hóa trị liệu nhắm mục tiêu hoặc liệu pháp miễn dịch. Một số bệnh nhân ung thư đại tràng giai đoạn 4 có mức độ lây lan hạn chế, đặc biệt là ở gan hoặc phổi, có thể phù hợp để phẫu thuật nhằm mục đích chữa bệnh/phá hủy tại chỗ kết hợp với hóa trị. Xạ trị có vai trò được xác định rõ ràng trước khi phẫu thuật trong ung thư trực tràng tiến triển tại chỗ, nhằm cải thiện khả năng kiểm soát tại chỗ và giảm tái phát tại chỗ. Phương pháp này cũng có thể được sử dụng để triệt các khu vực di căn khó mổ của ung thư.